
A flail chest describes when a segment of the rib cage breaks due to blunt thoracic trauma, high speed motor vehicle crash and becomes unattached from the chest wall. It can occur when 3 or more ribs are broken in at least two places, although not everyone with type of injury will develop a flail chest. However, if these injuries cause a segment of the chest to move independently, the generation of negative intrapleural pressure indicates a true paradoxical flail segment. This condition is of clinical significance in elderly patients or patients who have chronic lung disease, associated with morbidity and mortality.
Pathophysiology
This pathology of rib fracture associated with decrease chest movement due to pain that reduces the tidal volume and may predispose to significant atelectasis, impaired gas exchange in the affected lung beneath the fractured rib, altered in breathing mechanism. All these contributing factors may predispose later to pneumonia and pulmonary secretions retention, paradoxical chest movement.
Types
- Complete
- Incomplete
- Physeal
Classification according to the nature of the fracture:
- Spiral
- Transverse
- Comminuted
- Compression
Associated Conditions
Pulmonary complications 48-72 hours after admission:
- Haemothorax
- Pneumothorax
- Atelectasis
- Pneumonia
- Pleural effusion
- Subcutaneous emphysema
- ARDS (Acute Respiratory Distress Syndrome)
- Pulmonary emboli
- Aspiration
- Lobar collapse
Risk factors for developing associated conditions:
- Patient >65 years old
- rib fractures >3 ribs
- History of chronic lung conditions or CVD
- Pre-injury anti-coagulant use
- SpO2 <90%
Clinical Presentation
The clinical presentation depends on the severity of the impact, size of the flail segment and to what extent lung affected. The patient may complain of severe chest wall pain and may have tachypnea. On close observation there may be paradoxical chest wall movement. On inspiration the flail segment will move inwards whilst the rest of the chest expands and on expiration the flail segment will move outwards whilst the rest of the chest contracts.
If the patient is mechanically ventilated or on Bilevel Positive Airway Pressure (BiPAP) it may be difficult to diagnose and may only become obvious after extubation.
Diagnostic Procedures
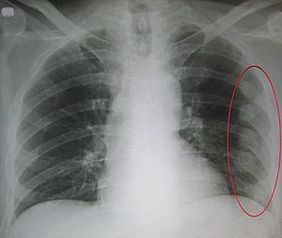
An abnormal chest movement during breathing may be a sign of flail chest.
Radiologists use Chest X-Rays to look for the following:
“Three or more adjacent ribs are fractured in two or more places. Clinically this can be a segment of only one or two ribs can act as a flail segment”
CT is more accurate modality in severe blunt trauma.
Outcome Measures
Medical Management
Medications
- Simple Analgesics
- Opioids like morphin when pain is not controlled with simple analgesics
- Patient Controlled Analgesia
- Operative fixation and Regional Anaesthetic
Surgery
- Regional anesthesia
- Serratus anterior block
- Paravertebral block
- Thoracic epidural
Internal Fixation
- It is a difficult and challenging procedure due to the nature of the rib.
- Decreases stay in ICU and MV duration.
- Incision site is Similar to thoracotomy and the latissmus dorsi muscle wasn't incised.
- Anterior fracture- plates and locking screws
- Posterior fracture - intramedullary splints
Physiotherapy Management
Role of chest physiotherapy for inpatient care depend on secretion clearance to prevent respiratory infection, restore normal lung volume, pulmonary function. There's still little information about physical therapy role after discharge from the hospital.
Management consists of the following:
- Ventilatory Management - supplemental oxygen therapy, continuous positive airway pressure or intubation if necessary
- CPAP - for negative intrapleural pressure and paradoxical movement, increases TV
- Open/closed suction if patient intubated.
- Pain Management and Education
- Education on fracture healing
- Early mobilization if possible to prevent contracture and loss of muscle mass
- Transfers to sitting out of bed
- Mobilization 2-3 times daily and SOOB 3-4 time/day
- Chest and airway clearance techniques (if inadequate)
- ACT: nebulizer with ACBT and education
- Bubble PEP or Flutter
- Deep breathing exercises and supported coughing technique
- Supported Cough: Wrap around technique or rolled up towel
- DBE/TEE’s with SMIs (2-4 secs hold)
- Positioning
- Positioning in side lying and high sitting
It was recommended to apply chest physiotherapy after adequate pain relief modalities
0Comments