
This guide provides a structured approach to abdominal X-ray interpretation and includes examples of relevant pathology.
Confirm details
Begin abdominal X-ray interpretation by checking the following details:
- Patient details: name, date of birth and unique identification number.
- Date and time the film was taken
- Previous imaging: useful for comparison.
 |
| Abdominal X-ray Interpretation |
Assess image type and quality
Projection of image
Assess the projection of the abdominal X-ray.
Typical projections of an abdominal X-ray include:
- Anterior-posterior (AP) supine
- Anterior-posterior (AP) erect
Exposure of image
Assess the X-ray to ensure the whole abdomen is visible from the level of the diaphragm to the pelvis.
Ensure the exposure is adequate to allow radiological assessment of both the small and large bowel.
Abdominal X-rays do not provide a good view of posterior abdominal structures due to overlying bowel and gas.
If bowel perforation is being considered, you don’t usually require an abdominal film, instead you need an erect chest X-ray, as this allows free gas under the diaphragm to be identified (the patient needs to have sat upright for at least 15-20 minutes prior to the X-ray to allow time for the air to rise).
A structured approach to interpretation
It’s important to have a systematic approach to interpreting abdominal X-rays as this decreases the risk of missing pathology.
In this guide we use the BBC approach:
- Bowel and other organs: small bowel, large bowel, lungs, liver, gallbladder, stomach, psoas muscles, kidneys, spleen and bladder.
- Bones: ribs, lumbar vertebrae, sacrum, coccyx, pelvis and proximal femurs.
- Calcification and artefact (e.g. renal stones)
Bowel and other organs
Small and large bowel
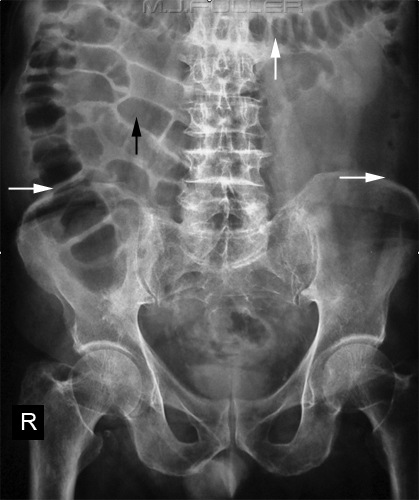
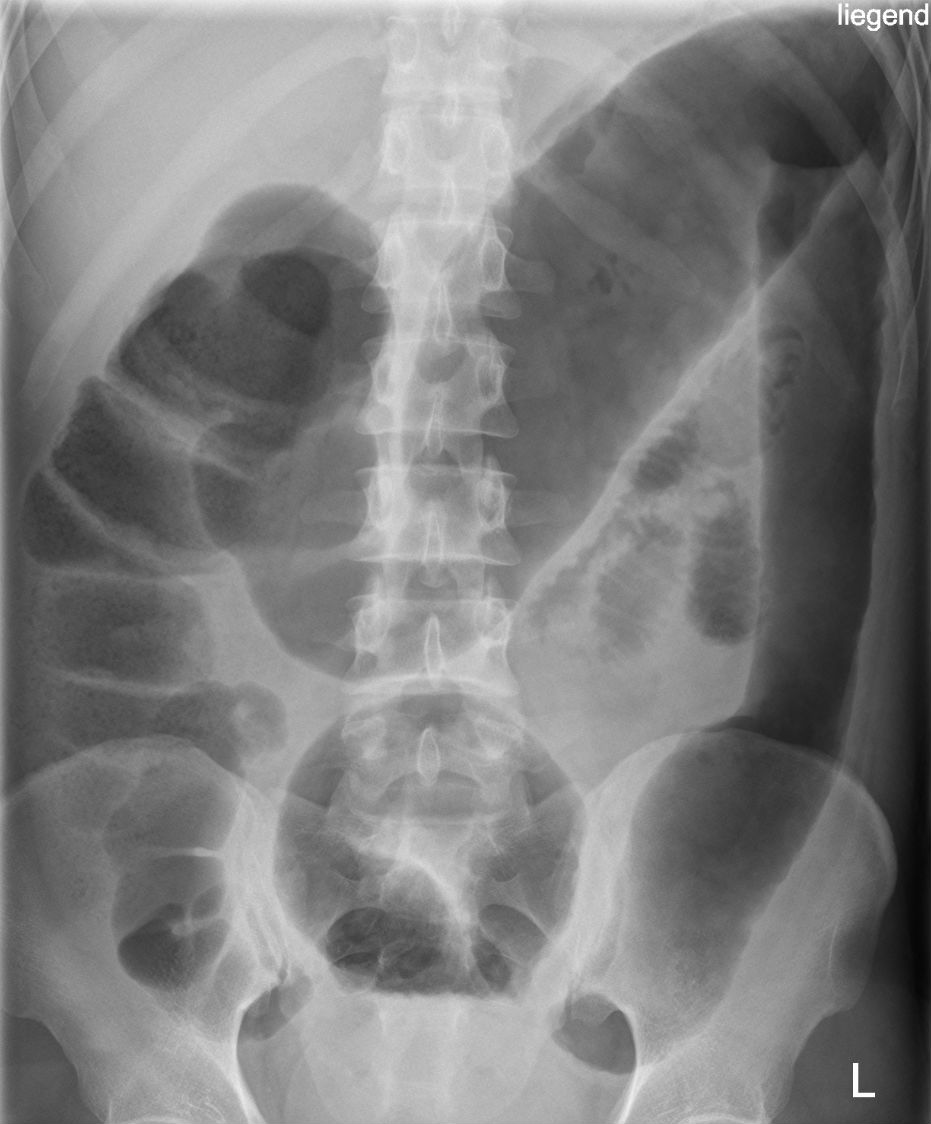
Differentiating between the small and large bowel on an abdominal X-ray is not always straightforward but there are a number of clues that may help you:
- The small bowel usually lies more centrally, with the large bowel framing it.
- The small bowel’s mucosal folds are known as valvulae conniventes and are visible across the full width of the bowel.
- The large bowel wall features pouches or sacculations that protrude into the lumen, known as haustra. In between the haustra are spaces known as plicae semilunaris. The haustra are thicker than the valvulae conniventes of the small bowel and typically do not appear to completely traverse the bowel. This distinction is unfortunately unreliable as dilated large bowel can have a haustral pattern that does, in fact, traverse the bowel.
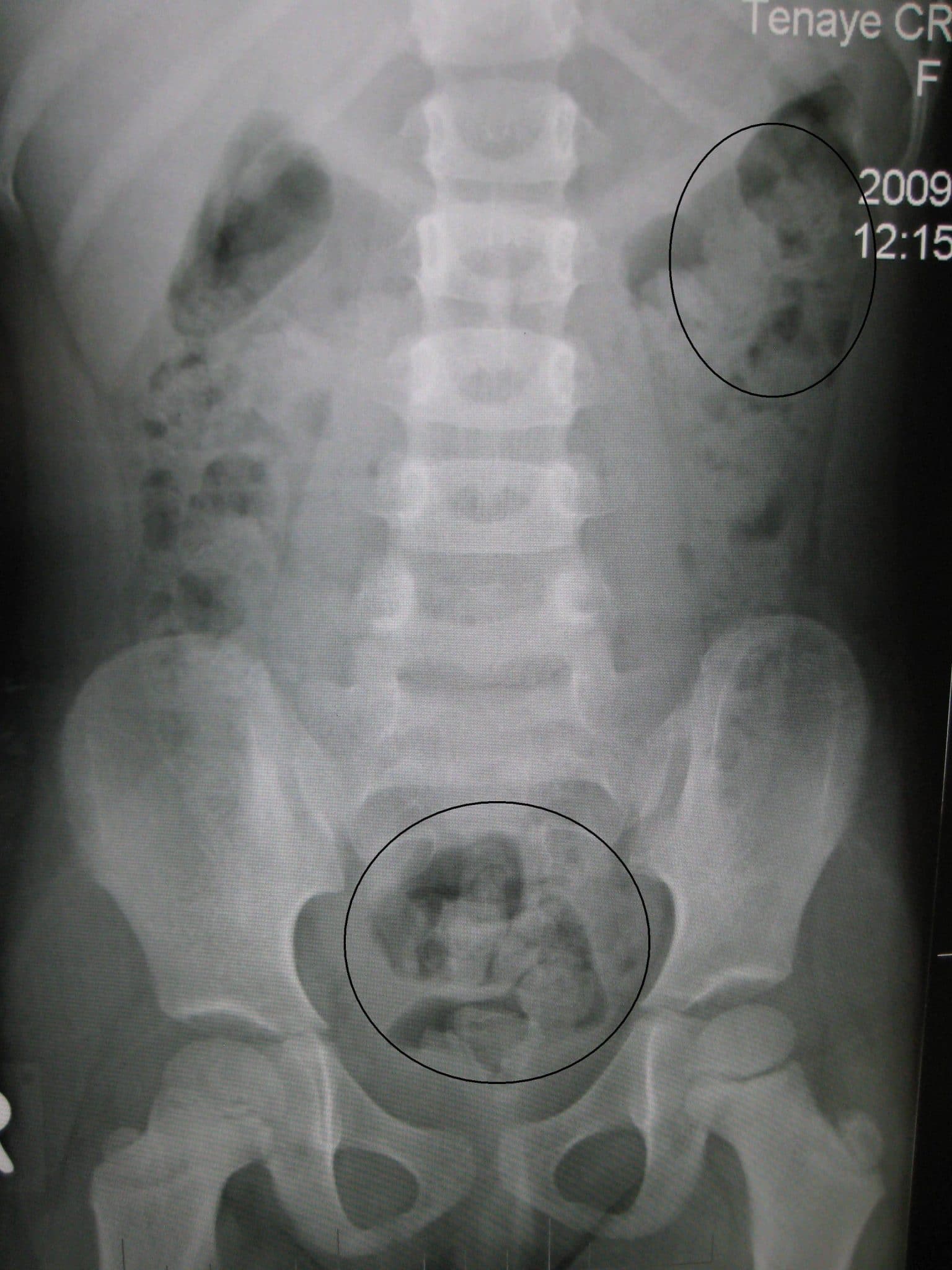
- Faeces have a mottled appearance and are most often visible in the colon, due to trapped gas within solid faeces.
Bowel diameter
The upper limits for the normal diameter of different bowel segments are as follows:
- Small bowel: 3cm
- Colon: 6 cm
- Caecum: 9 cm
This is often referred to as the ‘3/6/9 rule’.
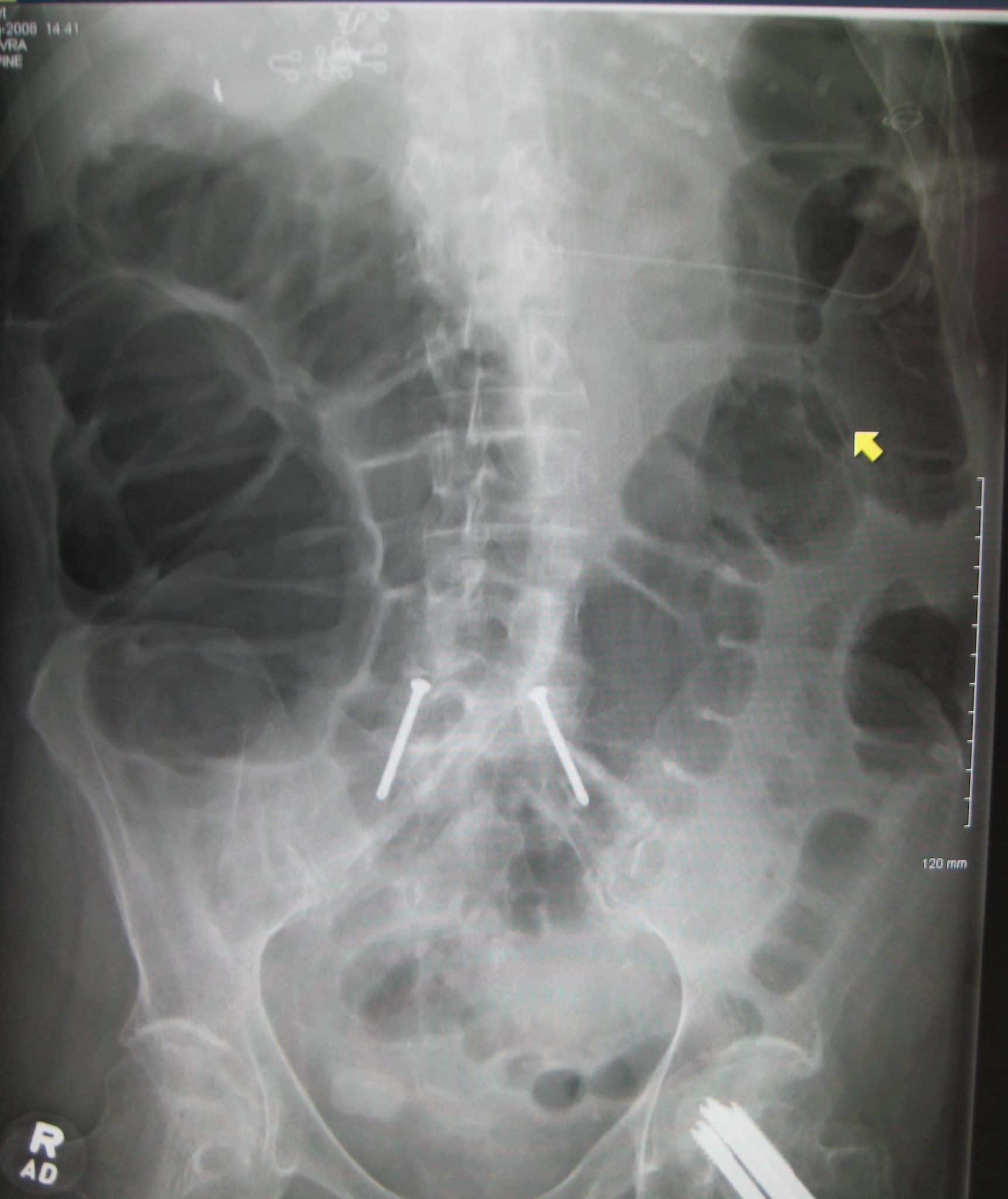
Typical abdominal X-ray features of small bowel obstruction include dilation of the small bowel (>3cm diameter) and much more prominent valvulae conniventes creating a ‘coiled-spring appearance‘.
Adhesions are the most common cause of small bowel obstruction in the developed world accounting for 75% of all cases. Some other causes include abdominal hernias (10%) and either intrinsic or extrinsic compression by neoplastic masses.
When interpreting an abdominal X-ray you should always inspect the inguinal regions, particularly if considering a hernia as a cause of small bowel obstruction, as they are often fairly obvious (even on plain abdominal X-rays).

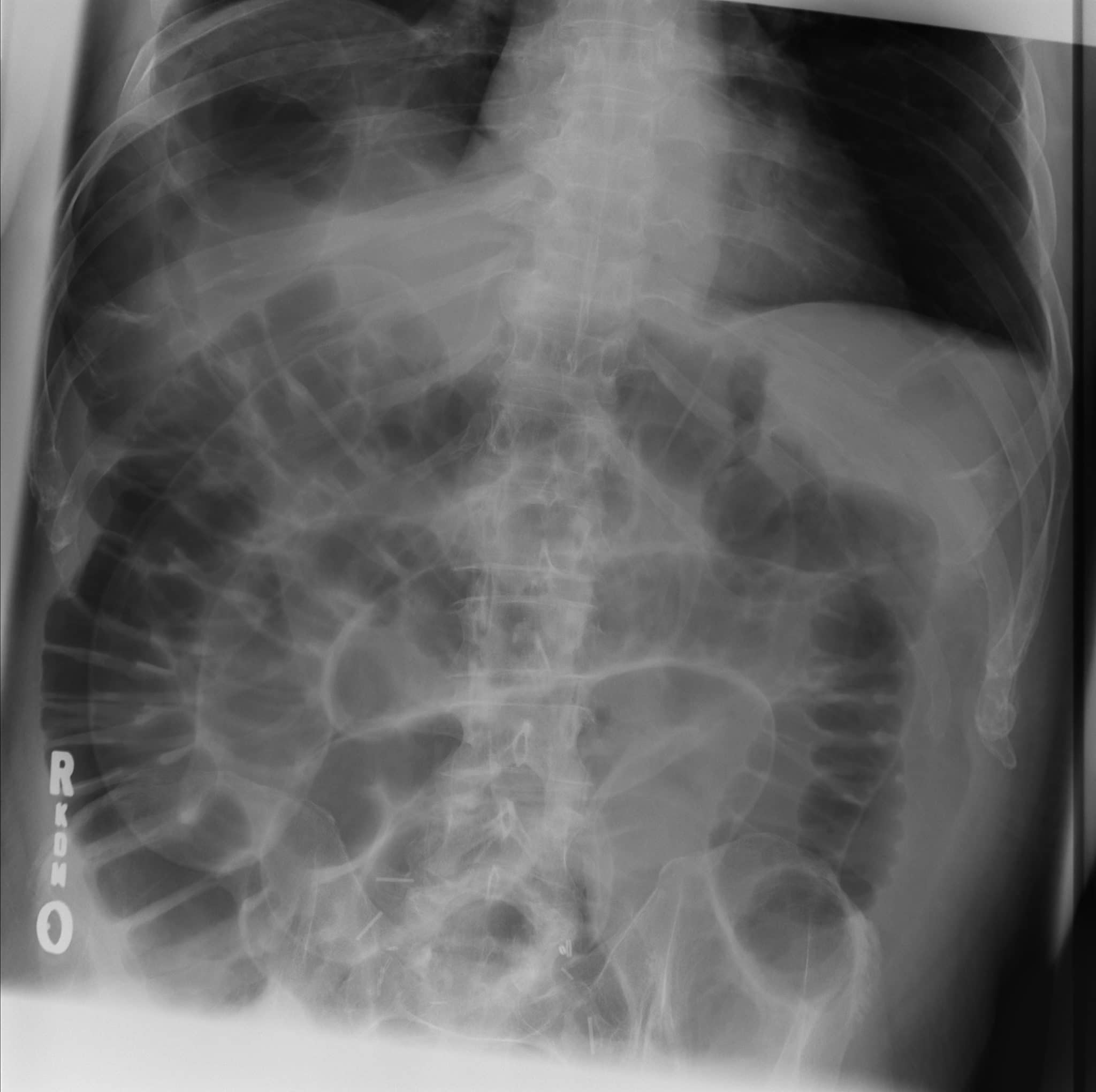
Large bowel obstruction
The most common causes of large bowel obstruction include colorectal carcinoma and diverticular strictures. Less common causes include hernias and volvulus.
Volvulus involves a twisting of the bowel on its mesentery and most commonly occurs at the sigmoid colon or caecum. Patients with volvulus are at high risk of bowel perforation and/or bowel ischaemia secondary to vascular compromise.
Typical abdominal X-ray findings in volvulus differ depending on the sub-type:
- Sigmoid volvulus: a characteristic ‘coffee bean’ appearance.
- Caecal volvulus: often described as having a fetal appearance.
Rigler’s (double wall) sign
In healthy individuals, only the inner wall of the bowel should be visible on an abdominal X-ray. The presence of free air within the abdomen (pneumoperitoneum) can result in both sides of the bowel wall becoming visible (this is known as Rigler’s sign).
Causes of pneumoperitoneum include a perforated abdominal viscus (e.g. perforated bowel, perforated duodenal ulcer) and recent abdominal surgery.
You should look closely for free air under the diaphragm on an erect chest X-ray if you suspect pneumoperitoneum.
Features of inflammatory bowel disease on abdominal X-ray include:
- Thumbprinting: mucosal thickening of the haustra due to inflammation and oedema causing them to appear like thumbprints projecting into the lumen.
- Lead-pipe (featureless) colon: loss of normal haustral markings secondary to chronic colitis.
- Toxic megacolon: colonic dilatation without obstruction associated with colitis.
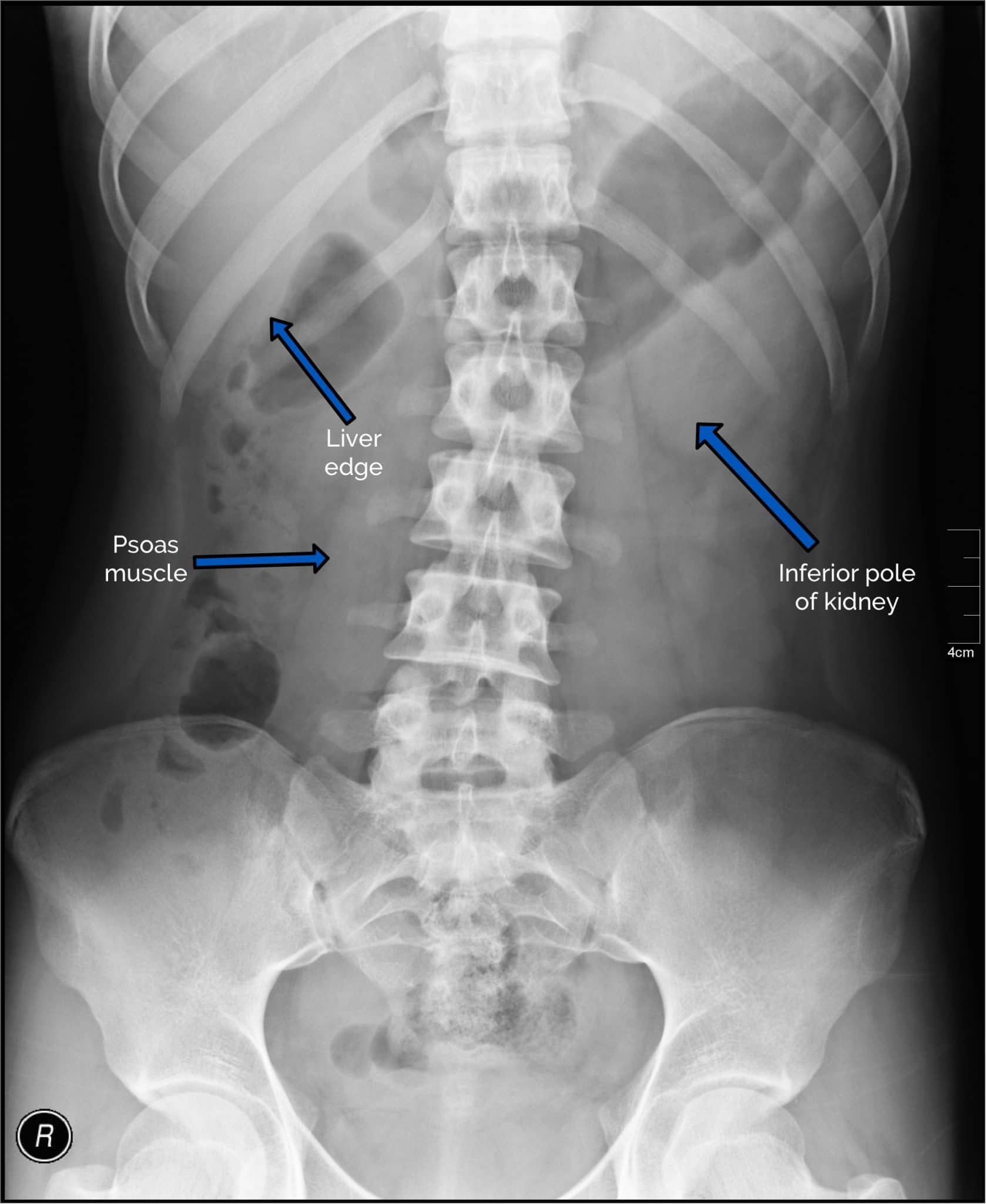
Other organs and structures
Although abdominal X-ray isn’t an ideal imaging modality for assessing the structures listed below, it’s useful to be able to recognise them to help orientate yourself and identify relevant pathology:
- Lungs: inspect the lung bases for pathology (e.g. consolidation) as abdominal pain can, in some cases, be caused by basal pneumonia.
- Liver: a large right upper quadrant structure.
- Gallbladder: rarely visible on an abdominal X-ray, however, you should quickly inspect for calcified gallstones and cholecystectomy clips.
- Stomach: visible between the left upper quadrant and midline, containing a variable amount of air.
- Psoas muscles: the lateral edge is marked by a relatively straight line either side of the lumbar vertebrae and sacrum.
- Kidneys: both are often visible, the right kidney is lower than the left due to the presence of the liver on the right.
- Spleen: located in the left upper quadrant, superior to the left kidney.
- Bladder: has a variable appearance depending on the fullness of the bladder.
Bones
Lots of bones are visible on an abdominal X-ray and it’s important that you can identify each and screen for pathology. In addition, bones on an abdominal X-ray provide useful landmarks which allow you to approximate the location of soft tissue structures (e.g. the ischial spines are the usual level of the vesicoureteric junction).
Bony structures commonly visible on abdominal X-ray include:
- Ribs
- Lumbar vertebrae
- Sacrum
- Coccyx
- Pelvis
- Proximal femurs
A wide range of bony pathologies can be identified on abdominal X-ray including fractures, osteoarthritis, Paget’s disease and bony metastases.

Calcification and artefact
Various high density (white) areas of calcification or artefact may be noted on abdominal X-ray including:
- Calcified gallstones in the right upper quadrant
- Renal stones/staghorn calculi
- Pancreatic calcification
- Vascular calcification
- Costochondral calcification
- Contrast (e.g. following a barium meal)
- Surgical clips
- Jewellery

Presenting an abdominal X-ray
Having a structured approach to summarising your findings is key to ensuring you communicate the salient points.
“This is a supine AP abdominal radiograph of Jayne Lister, date of birth 11th April 1970. The film is of good quality with adequate exposure. No prior imaging is available for comparison. Both the small and large bowel appear within normal limits. Other abdominal viscera appear normal within the limits of this projection. No obvious bony pathology is identified. No abnormal calcification is visible. In summary, this is a normal plain radiograph of the abdomen.”
Reviewer
Dr Kunal Patel
Radiology Registrar
References
- James Heilman, MD. Large bowel obstruction. Licence: CC BY-SA 3.0.
- Scott1751. Rigler’s sign. Licence: CC BY-SA 3.0.
- W. H. Liao, S. H. Lin, T. T. Wu. A 70-year-old male having advanced prostate cancer presenting with hypercalcemia and diffuse osteoblastic bone metastases: a case report. Cases Journal, Band 2, Nummer 1, 2009. Licence: CC-by-2.0.
- Nevit Dilman. Staghorn calculus. Licence: CC BY-SA 3.0.
- Wikiradiography. Differentiating large and small bowel. Licence: CC BY-SA 3.0.
- Hellerhoff. Toxic megacolon. Licence: CC BY-SA 3.0.
- James Heilman, MD. Constipation. Licence: CC BY-SA 3.0.
- James Heilman, MD. Volvulus. Licence: CC BY-SA 3.0.
- Fitzgerald, J. Edward F. (2010). Small Bowel Obstruction. Oxford: Wiley-Blackwell. pp. 74–79.
0Comments