
Allergy patch testing is used to screen substances to determine the cause of an allergic skin reaction. Patches with different suspected irritants (allergens) are applied to a person’s back and left in place for 48 hours. The skin is then examined for any signs of a hypersensitive reaction.
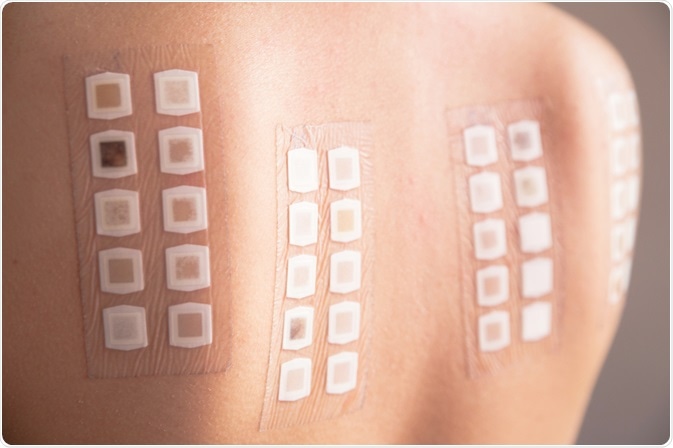
Image Credit: Neeila / Shutterstock.com
Patch testing detects allergic contact dermatitis, which is a type IV hypersensitivity reaction. Notably, this allergy test cannot be used to identify the cause of urticaria (hives) or food allergy.
Prick testing is another method used to test for a different type of allergy (type I) associated with hay fever, asthma, and contact urticaria. This method instead involves pricking the skin with a needle in order to test the blood and can be read after just 20 minutes.
What substances are tested?
The types of allergens tested in an allergy patch test include hair dye, preservatives, cosmetics, and medications. A standard set of allergens, such as those described in the European Standard Series of allergens, are applied to almost every patient, as these are the most common causes of dermatitis in about 85% of cases.
A variety of other compounds, which are often tailored to the patient, are also applied. To this end, the patient may bring their own materials from home or work to determine whether these materials are causing their reactions. The optimum concentration for each substance has been predetermined in order to induce an allergic reaction in susceptible skin without irritating skin that is not allergic.
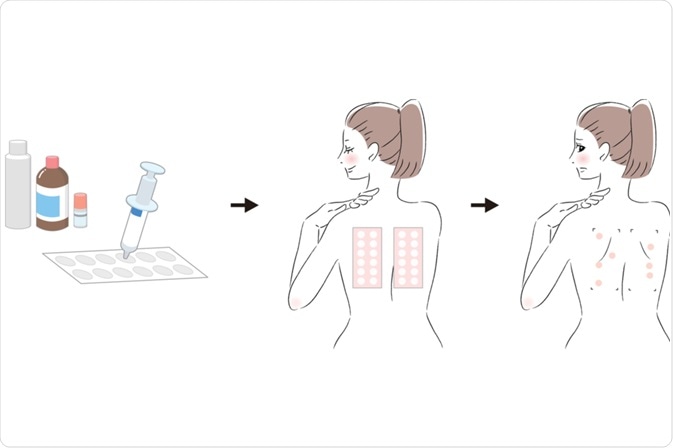
Image Credit: mucchanpapa / Shutterstock.com
Patch testing can also be helpful in determining the cause and pathophysiological mechanisms of cutaneous adverse drug reactions (CADR). The clinical relevance depends on the drug involved and the type of CADR investigated.
Ideally, this patch test will be used to determine the causes of generalized eczema, systemic contact dermatitis, maculopapular rash, acute generalized exanthematous pustulosis, and fixed drug eruption. Approximately 32-50% of drug patch tests are positive in patients who have developed a CADR.
Testing schedule
Day 1: Plastic or round aluminum square chambers, each containing small amounts of each substance, are applied to the patient’s upper back and secured with hypoallergenic tape.The general format for a patch test is as follows:
- After 48 hours: Patches are removed and the skin evaluated for reactivity.
- After 96 hours: A second assessment is performed, and evaluations determined.
An additional assessment may be required after 7 to 10 days in some people.
Results
Interpretation of skin reactions requires a good deal of experience and training. It is important to distinguish between irritation and an allergic reaction. The former occurs after the patch is removed but will reduce over the following day, whereas an allergic reaction will develop over several days and is more prominent on day five rather than immediately following patch removal.
The types of reactions observed in an allergy patch test may include:
- Negative
- Irritant reaction, e.g., a burn-like rash or follicular pustules
- Uncertain, due to the presence of a pink area under the test chamber.
- Weakly positive – slightly elevated pink or red plaques
- Strongly positive – marked by papules and vesicles
- Extreme – shown as blisters or ulcers
Patch tests may not always be conclusive. False negatives, in which no reaction arises despite an underlying allergy, as well as false positives, which indicate an allergy when there is not one, can occur. Patients can react differently to substances during a test than in everyday exposure, or to the same test performed at different times.
problems
A positive reaction causes an area of itchy, active dermatitis at the site of patch application. This is usually treated with topical steroids.
Other potential reactions include:
- Provocation of dermatitis in other areas outside of the patch site
- Sensitivity to the tape used
- “Angry back” usually in patients with active dermatitis before testing commenced or in those who experience many strong positive reactions. This results in many false positives to the tested substances.
- Generation of sensitivity to a new allergen (rare), which occurs approximately 10 days following testing
- Reactivation of the original rash, with dermatitis becoming more widespread
- Darker skin may develop dark patches that persist for many weeks/months
- These complications may make the interpretation of test results difficult. Therefore, retesting may be required, sometimes one allergen at a time, to confirm the results.
Medications can also interfere with the results of a patch test. Different drugs can either suppress or increase the risk of developing allergic reactions, which reduces the accuracy of the test. These drugs can include antihistamines, tricyclic antidepressants, heartburn medications, and the asthma medication omalizumab. Patients may need to stop taking medications for up to 10 days before a patch test, depending on how quickly they are cleared from the system.
Aftercare
By understanding the cause of their allergic dermatitis, patients can proceed with reducing symptoms or eliminating potential triggers of their symptoms. Treatment management plans may consist of medications, immunotherapy, dietary changes, and/or alterations to their work or home environment.
References
- https://www.dermnetnz.org/topics/patch-tests/
- https://www.mayoclinic.org/tests-procedures/allergy-tests/about/pac-20392895
- https://www.dermcoll.edu.au/atoz/allergy-patch-testing/
- Barbaud A. Drug patch testing in systemic cutaneous drug allergy. Toxicology 2005;209(2):209-216.
0Comments